Free Immunization Record PDF Form
Free Immunization Record PDF Form
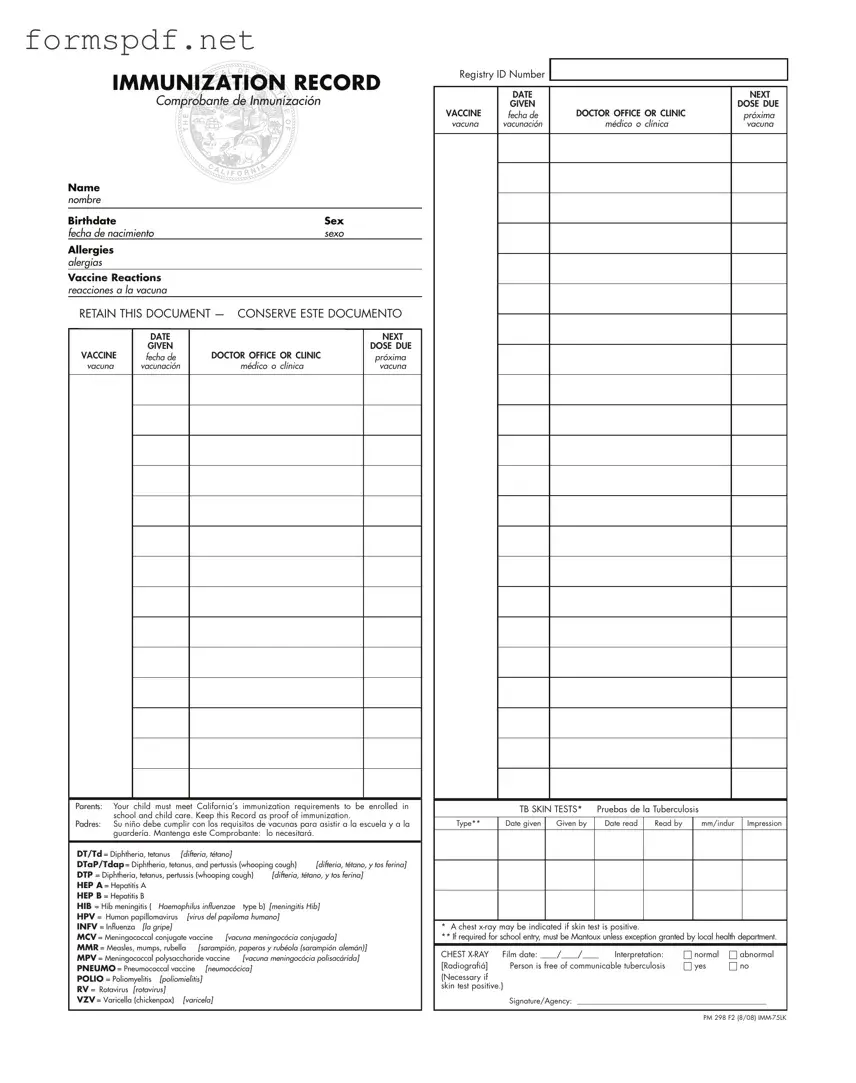
IMMUNIZATION RECORD
Comprobante de Inmunización
Name nombre
Birthdate |
|
|
Sex |
||
fecha de nacimiento |
|
sexo |
|||
Allergies |
|
|
|
|
|
alergias |
|
|
|
|
|
Vaccine Reactions |
|
|
|
|
|
reacciones a la vacuna |
|
|
|
|
|
RETAIN THIS DOCUMENT — CONSERVE ESTE DOCUMENTO |
|||||
|
DATE |
|
|
NEXT |
|
|
|
|
|||
|
GIVEN |
|
|
DOSE DUE |
|
VACCINE |
fecha de |
DOCTOR OFFICE OR CLINIC |
|
próxima |
|
vacuna |
vacunación |
médico o clínica |
|
vacuna |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Parents: Your child must meet California’s immunization requirements to be enrolled in school and child care. Keep this Record as proof of immunization.
Padres: Su niño debe cumplir con los requisitos de vacunas para asistir a la escuela y a la guardería. Mantenga este Comprobante: lo necesitará.
DT/Td = Diphtheria, tetanus |
[difteria, tétano] |
|
|
|
|
DTaP/Tdap = Diphtheria, tetanus, and pertussis (whooping cough) |
[difteria, tétano, y tos ferina] |
||||
DTP = Diphtheria, tetanus, pertussis (whooping cough) |
[difteria, tétano, y tos ferina] |
||||
HEP A = Hepatitis A |
|
|
|
|
|
HEP B = Hepatitis B |
|
|
|
|
|
HIB = Hib meningitis ( |
Haemophilus influenzae |
type b) |
[meningitis Hib] |
||
HPV = Human papillomavirus |
[virus del papiloma humano] |
|
|||
INFV = Influenza [la gripe] |
|
|
|
|
|
MCV = Meningococcal conjugate vaccine [vacuna meningocócia conjugada] |
|||||
MMR = Measles, mumps, rubella [sarampión, paperas y rubéola (sarampión alemán)] |
|||||
MPV = Meningococcal polysaccharide vaccine |
[vacuna meningocócia polisacárida] |
||||
PNEUMO = Pneumococcal vaccine [neumocócica] |
|
|
|||
POLIO = Poliomyelitis |
[poliomielitis] |
|
|
|
|
RV = Rotavirus [rotavirus] |
|
|
|
|
|
VZV = Varicella (chickenpox) |
[varicela] |
|
|
|
|
Registry ID Number
|
DATE |
|
NEXT |
|
GIVEN |
|
DOSE DUE |
VACCINE |
fecha de |
DOCTOR OFFICE OR CLINIC |
próxima |
vacuna |
vacunación |
médico o clínica |
vacuna |
|
TB SKIN TESTS* |
Pruebas de la Tuberculosis |
|
|
|||
|
|
|
|
|
|
|
|
Type** |
Date given |
Given by |
Date read |
Read by |
|
mm/indur |
Impression |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
* A chest
** If required for school entry, must be Mantoux unless exception granted by local health department.
CHEST |
Film date: ____/____/____ |
Interpretation: |
|
normal |
|
abnormal |
|
[Radiografiá] |
Person is free of communicable tuberculosis |
|
yes |
|
|
no |
|
|
|
|
|||||
(Necessary if skin test positive.)
Signature/Agency: __________________________________________________
PM 298 F2 (8/08)
Living Will Downloadable 5 Wishes Printable Version - The Five Wishes document lets you define who will make health care decisions for you if you're unable to do so yourself.
This Independent Contractor Agreement is crucial for businesses looking to establish clear working parameters, ensuring a smooth engagement process. It details obligations and expectations of both parties, making it important to have a comprehensive understanding of the "Florida Independent Contractor Agreement" before proceeding. For more information, click here: Florida Independent Contractor Agreement form overview.
Printable Return to Work Doctors Note - Collect necessary information for work release approval.
How to Apply for Asylum in Usa - The I-589 form can be a vital step towards obtaining legal residency.