Free DD 2870 PDF Form
Free DD 2870 PDF Form
Prescribed by: DoDM 6025.18 |
CONTROLLED when filled |
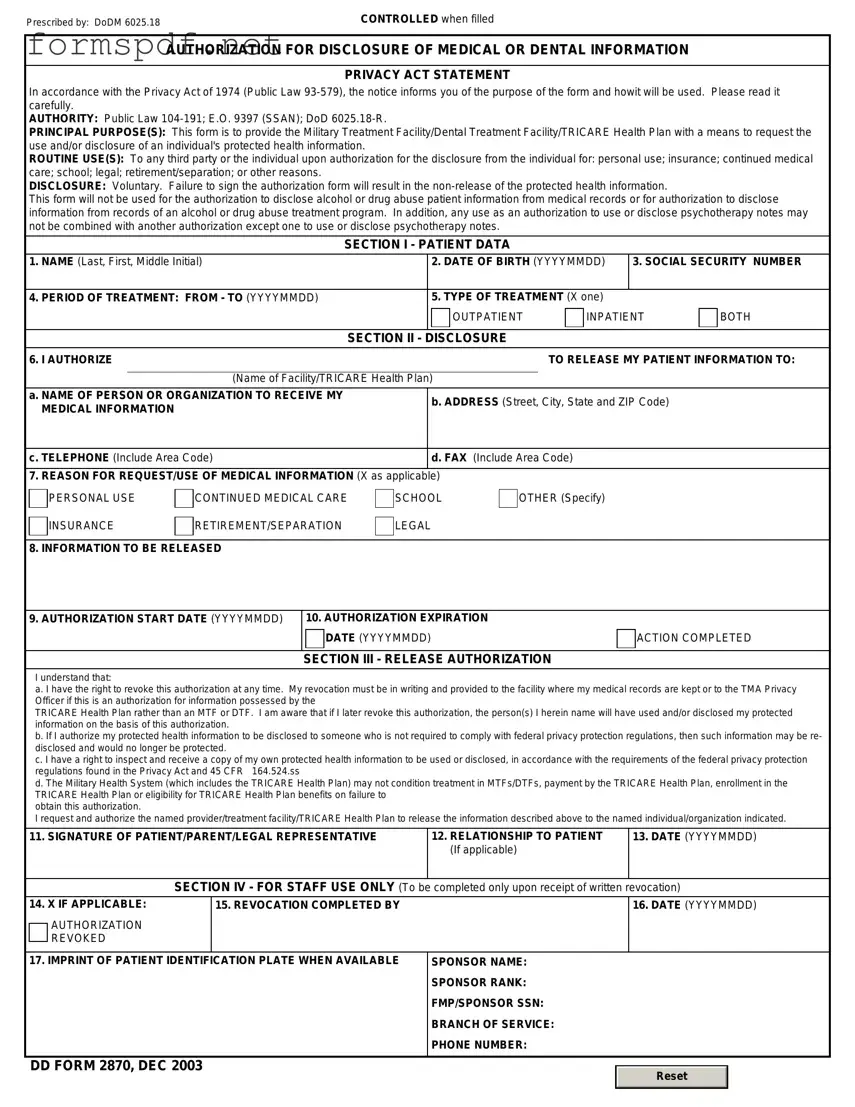
AUTHORIZATION FOR DISCLOSURE OF MEDICAL OR DENTAL INFORMATION
PRIVACY ACT STATEMENT
In accordance with the Privacy Act of 1974 (Public Law
AUTHORITY: Public Law
PRINCIPAL PURPOSE(S): This form is to provide the Military Treatment Facility/Dental Treatment Facility/TRICARE Health Plan with a means to request the use and/or disclosure of an individual's protected health information.
ROUTINE USE(S): To any third party or the individual upon authorization for the disclosure from the individual for: personal use; insurance; continued medical care; school; legal; retirement/separation; or other reasons.
DISCLOSURE: Voluntary. Failure to sign the authorization form will result in the
This form will not be used for the authorization to disclose alcohol or drug abuse patient information from medical records or for authorization to disclose information from records of an alcohol or drug abuse treatment program. In addition, any use as an authorization to use or disclose psychotherapy notes may not be combined with another authorization except one to use or disclose psychotherapy notes.
SECTION I - PATIENT DATA
1. NAME (Last, First, Middle Initial) |
|
2. DATE OF BIRTH (YYYYMMDD) |
3. SOCIAL SECURITY NUMBER |
|||
|
|
|
|
|
|
|
4. PERIOD OF TREATMENT: FROM - TO (YYYYMMDD) |
|
5. TYPE OF TREATMENT (X one) |
|
|
||
|
|
|
OUTPATIENT |
INPATIENT |
BOTH |
|
|
|
|
|
|
|
|
|
|
SECTION II - |
DISCLOSURE |
|
|
|
6. I AUTHORIZE |
|
|
TO RELEASE MY PATIENT INFORMATION TO: |
|||
|
|
|
|
|
||
|
(Name of Facility/TRICARE Health Plan) |
|
|
|
||
a. NAME OF PERSON OR ORGANIZATION TO RECEIVE MY |
|
b. ADDRESS (Street, City, State and ZIP Code) |
|
|||
MEDICAL INFORMATION |
|
|
||||
|
|
|
|
|
||
|
|
|
|
|
||
c. TELEPHONE (Include Area Code) |
|
d. FAX (Include Area Code) |
|
|
||
|
|
|
|
|
||
7. REASON FOR REQUEST/USE OF MEDICAL INFORMATION (X as applicable) |
|
|
|
|
||
PERSONAL USE
INSURANCE
CONTINUED MEDICAL CARE
RETIREMENT/SEPARATION
SCHOOL
LEGAL
OTHER (Specify)
8. INFORMATION TO BE RELEASED
9. AUTHORIZATION START DATE (YYYYMMDD)
10. AUTHORIZATION EXPIRATION
DATE (YYYYMMDD)
SECTION III - RELEASE AUTHORIZATION
ACTION COMPLETED
I understand that:
a. I have the right to revoke this authorization at any time. My revocation must be in writing and provided to the facility where my medical records are kept or to the TMA Privacy Officer if this is an authorization for information possessed by the
TRICARE Health Plan rather than an MTF or DTF. I am aware that if I later revoke this authorization, the person(s) I herein name will have used and/or disclosed my protected information on the basis of this authorization.
b. If I authorize my protected health information to be disclosed to someone who is not required to comply with federal privacy protection regulations, then such information may be re- disclosed and would no longer be protected.
c. I have a right to inspect and receive a copy of my own protected health information to be used or disclosed, in accordance with the requirements of the federal privacy protection regulations found in the Privacy Act and 45 CFR 164.524.ss
d. The Military Health System (which includes the TRICARE Health Plan) may not condition treatment in MTFs/DTFs, payment by the TRICARE Health Plan, enrollment in the TRICARE Health Plan or eligibility for TRICARE Health Plan benefits on failure to
obtain this authorization.
I request and authorize the named provider/treatment facility/TRICARE Health Plan to release the information described above to the named individual/organization indicated.
11. SIGNATURE OF PATIENT/PARENT/LEGAL REPRESENTATIVE |
12. RELATIONSHIP TO PATIENT |
13. DATE (YYYYMMDD) |
|
(If applicable) |
|
|
|
|
SECTION IV - FOR STAFF USE ONLY (To be |
completed only upon receipt of written revocation) |
|
14. X IF APPLICABLE:
AUTHORIZATION REVOKED
15. REVOCATION COMPLETED BY
16.DATE (YYYYMMDD)
17. IMPRINT OF PATIENT IDENTIFICATION PLATE WHEN AVAILABLE |
SPONSOR NAME: |
||
|
SPONSOR RANK: |
||
|
FMP/SPONSOR SSN: |
||
|
BRANCH OF SERVICE: |
||
|
PHONE NUMBER: |
||
|
|
|
|
DD FORM 2870, DEC 2003 |
|
|
|
|
Reset |
|
|
|
|
|
|
|
|
|
|
Fedx Freight - The form includes customer service contact information.
A Rental Application form is an essential document that potential tenants complete to express their interest in renting a property. This form provides landlords with vital information about the applicants, including their financial standing and rental history. Understanding how to fill out this form accurately can significantly enhance your chances of securing your desired rental—start by completing the application below, available at pdftemplates.info/rental-application-form/.
Pay Stub for Independent Contractor - Aids in promoting timely payment practices for contractors.