Free 680 PDF Form
Free 680 PDF Form

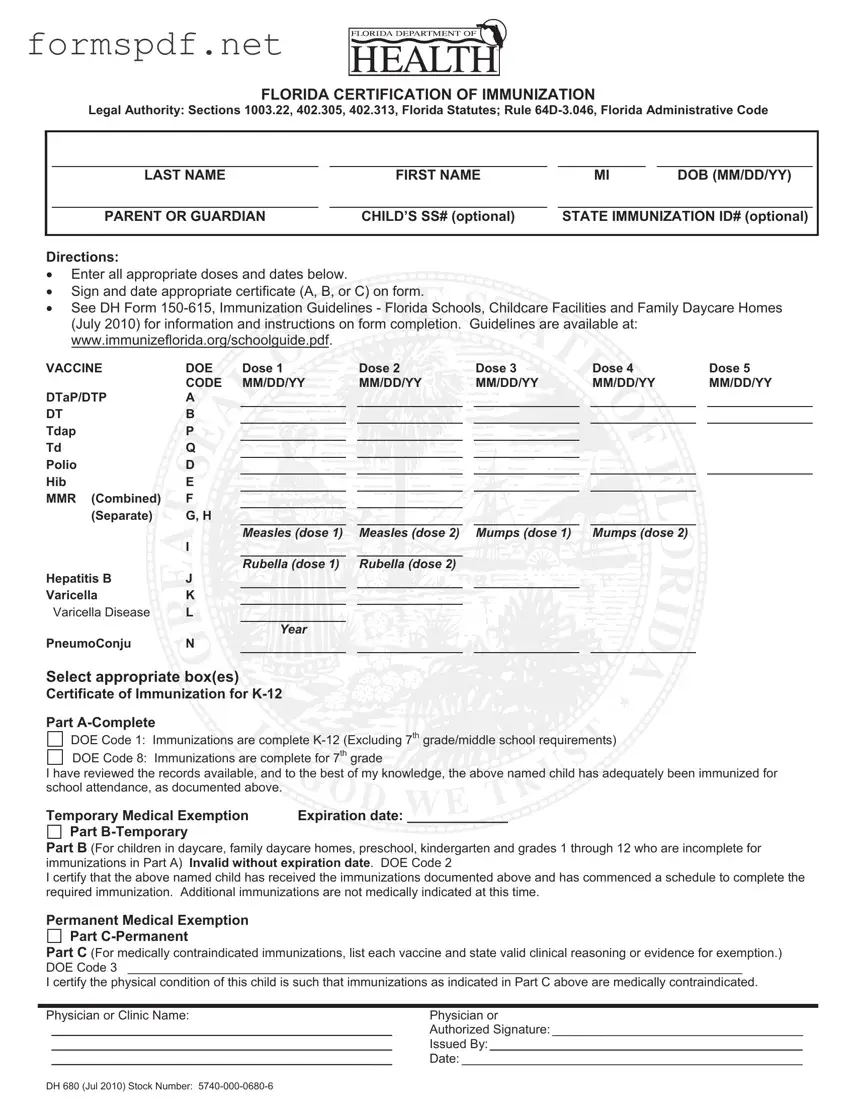
FLORIDA CERTIFICATION OF IMMUNIZATION
Legal Authority: Sections 1003.22, 402.305, 402.313, Florida Statutes; Rule
|
|
|
|
|
|
|
|
|
|
LAST NAME |
|
FIRST NAME |
|
MI |
|
DOB (MM/DD/YY) |
|
|
|
|
|
|
|
|
|
|
|
PARENT OR GUARDIAN |
|
CHILD’S SS# (optional) |
|
STATE IMMUNIZATION ID# (optional) |
|
||
|
|
|
|
|
|
|
|
|
Directions:
Enter all appropriate doses and dates below.
Sign and date appropriate certificate (A, B, or C) on form.
or C) on form.
See DH Form 










VACCINE |
DOE |
Dose 1 |
|
Dose 2 |
|
Dose 3 |
|
Dose 4 |
|
Dose 5 |
|
CODE |
MM/DD/YY |
|
MM/DD/YY |
|
MM/DD/YY |
|
MM/DD/YY |
|
MM/DD/YY |
DTaP/DTP |
A |
|
|
|
|
|
|
|
|
|
DT |
B |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
Tdap |
P |
|
|
|
|
|
|
|
|
|
Td |
Q |
|
|
|
|
|
|
|
|
|
Polio |
D |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
Hib |
E |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
MMR (Combined) |
F |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
(Separate) |
G, H |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
Measles (dose 1) |
|
Measles (dose 2) |
|
Mumps (dose 1) |
|
Mumps (dose 2) |
|
|
|
I |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Rubella (dose 1) |
|
Rubella (dose 2) |
|
|
|
|
|
|
Hepatitis B |
J |
|
|
|
|
|
|
|
|
|
Varicella |
K |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
Varicella Disease |
L |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Year
PneumoConju N
Select appropriate box(es)
box(es)
Certificate of Immunization  K-12
K-12
Part
DOE Code 1: Immunizations are complete
DOE Code 8: Immunizations are complete for 7th grade
are complete for 7th grade
I have reviewed the records available, and to the best of my knowledge, the above named child has adequately been immunized for school attendance, as documented above.
and to the best of my knowledge, the above named child has adequately been immunized for school attendance, as documented above.


Temporary Medical Exemption |
Expiration date: _____________ |
Part |
|
Part B (For children in daycare, family daycare homes, preschool, kindergarten and grades 1 through 12 who are incomplete for immunizations in Part A) Invalid without expiration date. DOE Code 2
I certify that the above named child has received the immunizations documented above and has commenced a schedule to complete the required immunization. Additional immunizations are not medically indicated at this time.
Permanent Medical Exemption
Part
Part C (For medically contraindicated immunizations, list each vaccine and state valid clinical reasoning or evidence for exemption.) DOE Code 3 ________________________________________________________________________________________
I certify the physical condition of this child is such that immunizations as indicated in Part C above are medically contraindicated.
Physician or Clinic Name: |
Physician or |
_________________________________________________ |
Authorized Signature: ____________________________________ |
_________________________________________________ |
Issued By:_____________________________________________ |
_________________________________________________ |
Date: _________________________________________________ |
DH 680 (Jul 2010) Stock Number:
Free Printable Direction to Pay Form - Using this form helps ensure the body shop can begin repairs without concern for payment delays.
For more information on how to access the necessary documents, you can visit pdftemplates.info/sample-tax-return-transcript-form/, which provides helpful resources related to the sample Tax Return Transcript form and its proper usage for various financial processes.
Da - Whether dealing with small items or large equipment, this form is indispensable.